The EHR that carried you through solo practice starts creaking the day you hire clinician number two. Suddenly there are two calendars that don’t talk to each other, an associate whose notes need your signature, and a payroll spreadsheet that eats your Sunday evening. The software didn’t get worse. Your practice changed shape.
This guide covers what an EHR for group practices has to do that solo tools don’t, how the per-seat pricing math actually works, and the part most scaling guides skip: the website side, because every clinician you hire needs a caseload, and caseloads come from somewhere.
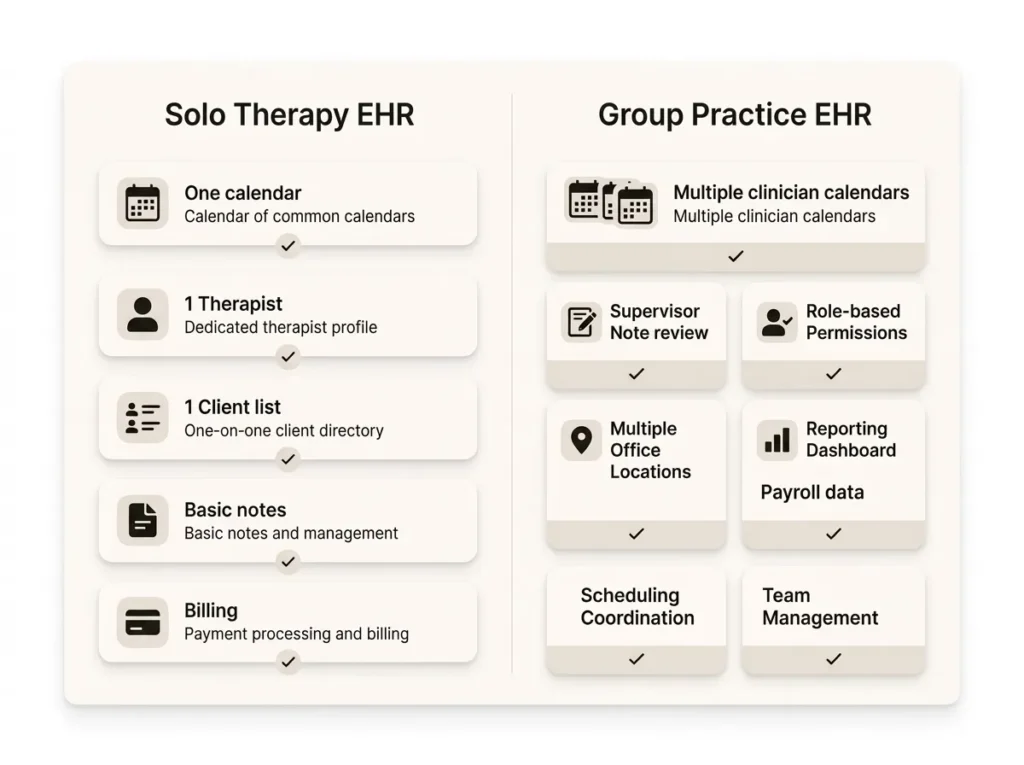
What an EHR for group practices does that solo tools don’t
An EHR for group practices adds four things solo tools lack: multi-clinician scheduling across locations and telehealth, supervisor note review with co-signing, role-based permissions for admin staff, and reporting that splits revenue and caseload by clinician. If any of that currently lives in a spreadsheet, you’ve already outgrown your system.
Most therapy EHRs technically support multiple clinicians. The question is whether they support them well. A platform designed for solo practitioners with group features bolted on will let you add seats, then quietly force the owner to become the human middleware connecting schedules, supervision, and payroll. Our guide to the best EHR systems for therapists covers which platforms were built for groups versus stretched into them.
Multi-clinician scheduling breaks first
Scheduling is usually the first thing that snaps. With one clinician, a calendar is a list. With five, it’s a routing problem: which clinician has openings, at which location, for which client type, covered by which insurance panel.
The features that matter once you’re a group:
- Per-clinician availability with separate telehealth and in-office blocks
- Client self-scheduling that routes correctly, so a new client books with the clinician who has room, not whoever’s listed first
- Room and location management if you share physical space
- Waitlist handling that fills cancellations without a phone-tag marathon
An opinion from watching group practices operate: turn client self-scheduling on. Solo therapists can get away with email back-and-forth. In a group, every manually booked session is admin payroll you’re spending to do what software does at 2 a.m. for free.
Supervisor co-signing, roles, and who sees what
The moment you bring on pre-licensed clinicians, your EHR becomes a supervision tool. Associates and interns write notes; supervisors review and co-sign them; the record has to show who wrote what and when, because your license is attached to their documentation.
Look for a real co-signing workflow: a queue of notes awaiting review, the ability to send one back with comments, and a locked audit trail once signed. If the “workflow” is your associate texting “can you sign my notes,” the EHR isn’t doing its job.
Role-based access matters just as much. Your front-desk person needs the schedule and billing status, not session notes. Your biller needs claims data, not psychotherapy notes. Granular permissions are how a group practice honors the minimum-necessary principle without daily judgment calls, and they’re a feature solo tools often lack entirely. Whatever platform you pick, confirm the vendor signs a BAA covering every user seat; HHS publishes sample business associate provisions if you want to see what one should contain.
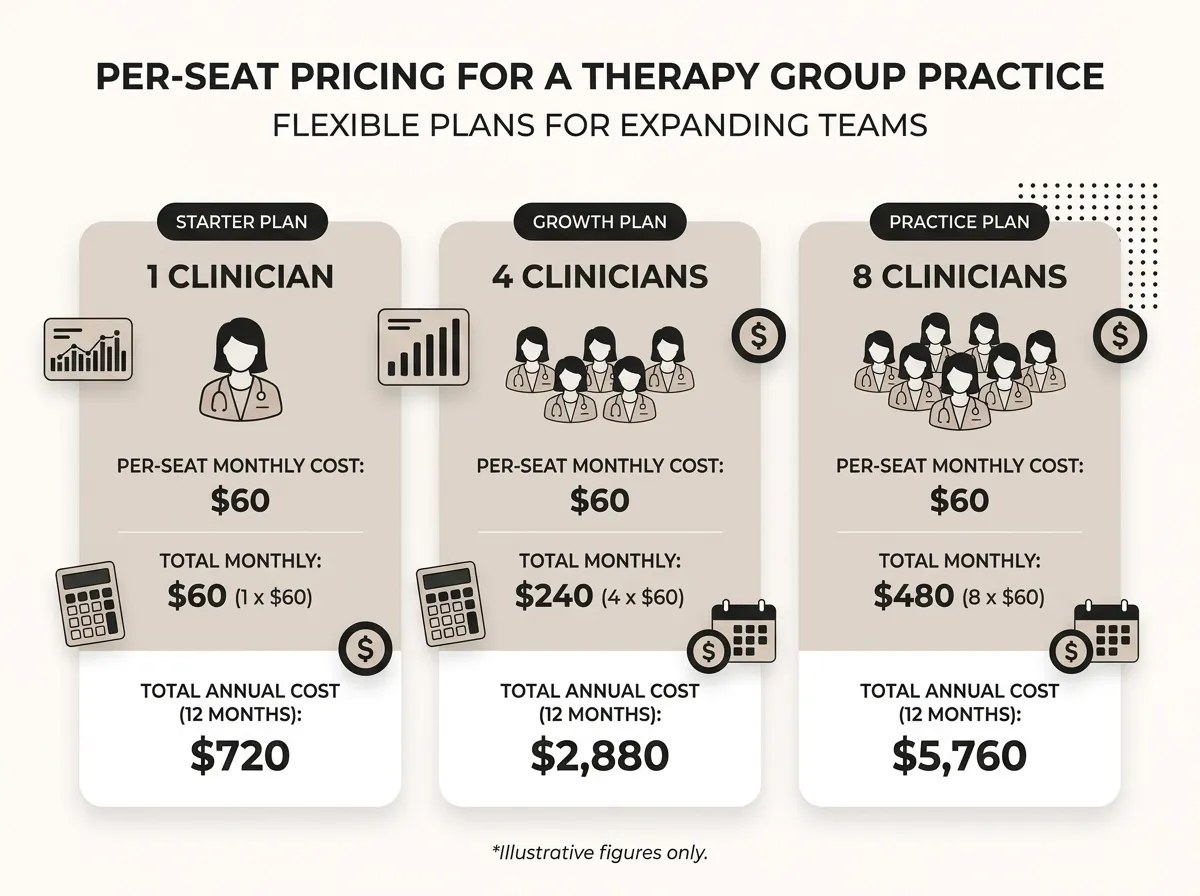
Run the per-seat pricing math before you sign
Nearly every therapy EHR prices per clinician per month. Some discount additional seats, some charge full price for each, and admin or scheduler seats are sometimes cheaper or free. Those details change the math more than the headline price does, so get them in writing.
The arithmetic itself is simple. Say a platform runs $60 per clinician per month, purely as an illustration: a solo pays $720 a year, while an eight-clinician group pays $5,760. At that scale a $10 per-seat difference between two vendors is nearly $1,000 a year, which is why groups should negotiate and solos mostly shouldn’t bother. For current real-world numbers, our therapy EHR cost breakdown tracks what the major platforms charge.
Here’s the trade-off nobody selling upgrades will volunteer: group-capable platforms cost more, and most of their features sit idle until you have three or more clinicians. If you’re a solo with one intern, upgrading early is paying rent on empty rooms. Wait until the second hire is actually signed.
Split billing, payroll, and the reports owners actually use
Group practice finances have a shape solo finances don’t: revenue comes in under multiple clinicians and goes out as splits, salaries, or 1099 payments. Your EHR won’t run payroll (none of them do it well, and you’ll still want an accountant or payroll tool), but it has to produce the numbers payroll depends on.
The reports worth demanding in a demo:
- Sessions and revenue by clinician, filterable by date range and payer
- Collections versus billed, so compensation is based on money received, not money hoped for
- Caseload and utilization per clinician, which tells you who has room and when to hire next
- Payer mix, because one insurer quietly becoming 60% of revenue is a risk you want to see coming
When those reports say your clinicians are full and referrals keep arriving, that’s a growth signal, and it’s the point where owners usually shift attention from operations to marketing. That transition is exactly what our private practice growth service exists for.
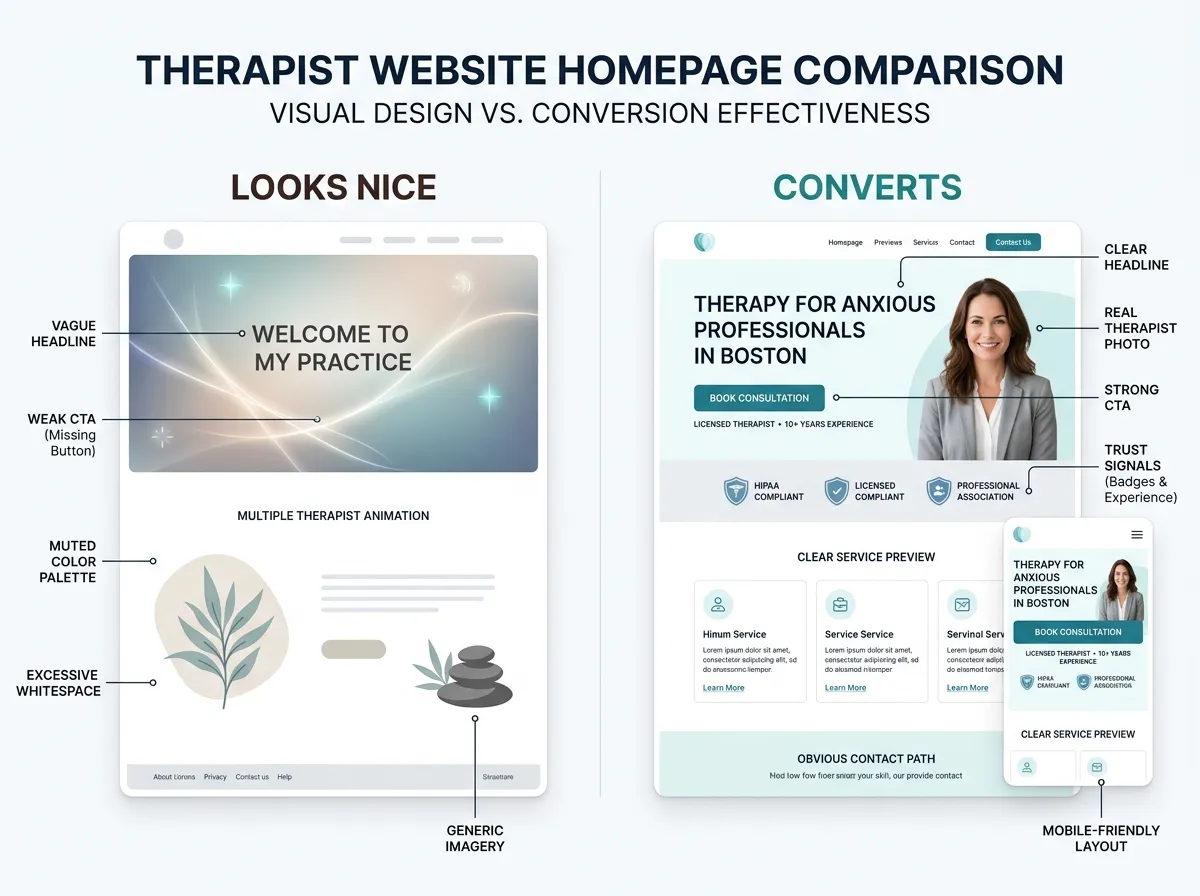
The website side of scaling: every clinician needs a page that converts
Here’s what the EHR guides leave out. Software manages the clients you have; it doesn’t create demand for the clinicians you just hired. A new associate with an empty caseload is the most expensive line item in a group practice, and the fastest fix lives on your website.
Every clinician needs a real bio page: photo, specialties, who they help, insurance accepted, and a direct booking path. Not a name in a grid. Prospective clients choose a person, not a practice, and a thin team page sends them back to the directories. We wrote a full guide on building a therapist About page that converts, and the same principles apply to every team bio.
Recruiting runs through the same pages. Strong clinicians research you before applying, and a practice that presents its team well signals it will market them well too. If you’re hiring, our post on career options in mental health pairs nicely with a careers page that actually sells the role.
FAQ: EHRs for group practices
What’s the best EHR for a mental health group practice?
How much does a group practice EHR cost per clinician?
Do admin staff need paid EHR seats?
When should a group practice switch EHRs?
Where to go from here
Pick the EHR that fits the practice you’re becoming, not the one you were. Then make sure your website can fill the caseloads your new system will manage. If your team is growing faster than your site, get a custom quote and we’ll map out what a group-practice website that converts actually looks like.