Short version: yes, and earlier than most guides admit. Not because the law demands software (it doesn’t), but because the alternative is stitching together five tools and a filing cabinet while you’re also trying to see clients, bill insurance, and remember which consent form is in which drawer.
Here’s the longer version, because the details decide whether that money is well spent in month one or wasted until month six. This is business guidance for practice owners, not legal advice; your licensing board and a healthcare attorney own the final word on your records setup.
So, do therapists need an EHR? The short answer
Do therapists need an EHR? Legally, no. Paper records can satisfy HIPAA and state board requirements if they’re stored securely. Practically, yes: once you add scheduling, reminders, notes, superbills, and telehealth, an EHR replaces four or five separate tools, and most new practices hit that point fast.
Our actual position, since “it depends” helps nobody: get the EHR before you see your first client. It’s one of the only subscriptions that earns its keep at a caseload of one, because your record-keeping obligations start with session one, not with client twenty. Setting up clean systems on day one costs an afternoon. Migrating a year of paper charts into software costs a week you won’t have.
What paper and spreadsheets can legally do
Paper gets more legal credit than the software industry likes to admit. HIPAA is format-neutral: a locked filing cabinet with a sign-out log can hold clinical records lawfully, and therapists ran practices that way for decades. State boards generally require that records exist, are complete, and are retained for a set period; most don’t mandate the container.
Spreadsheets and cloud docs are where people get into trouble. A client list in a free Google or Microsoft account means PHI sitting with a vendor that hasn’t signed a BAA, which is a HIPAA problem regardless of how strong your password is. Some paid business plans of those platforms will sign a BAA for covered services; the free consumer versions won’t.
One nuance worth knowing: HIPAA technically applies to providers who transmit health information electronically for covered transactions, like electronic insurance claims. A strictly cash-pay therapist who never bills electronically may not be a covered entity at all — HHS explains who counts. But state privacy law and your ethics code still apply, and building your practice as if HIPAA covers you is the only sensible default. Confirm your specific status with your board or an attorney rather than guessing.
So paper is legal. What it can’t do is send appointment reminders, generate a superbill, or let a client book online at 11 p.m., which is when a lot of therapy-seekers finally sit down to look.
The real threshold where an EHR pays for itself
Forget caseload counts for a second and look at your task mix.
If you take insurance, the threshold is your first claim. Filing, tracking, and resubmitting claims by hand is miserable at any volume, and billing features alone justify the subscription. Our therapy EHR cost guide breaks down what the platforms charge, but even the pricier options cost less per month than one unpaid claim that slipped through the cracks.
Self-pay practices have a softer threshold, and here’s where the honest math lives. Count what each client actually generates: scheduling messages, a reminder, a session note, an invoice or superbill, a telehealth link. Handle each step manually and a small caseload quietly produces an hour or more of weekly admin. Price that hour at your session rate and the subscription looks cheap. In our view, five recurring clients is roughly where hand-run admin starts costing more than software, and almost everyone crosses that line sooner than they planned to.
There’s a compliance dividend too. An EHR that signs a BAA gives you encrypted storage, access logs, and backups by default. Recreating that discipline with paper and consumer tools is possible, but you become the compliance system, and you’re already the clinician, the biller, and the marketer.
EHR first or website first? The sequencing answer
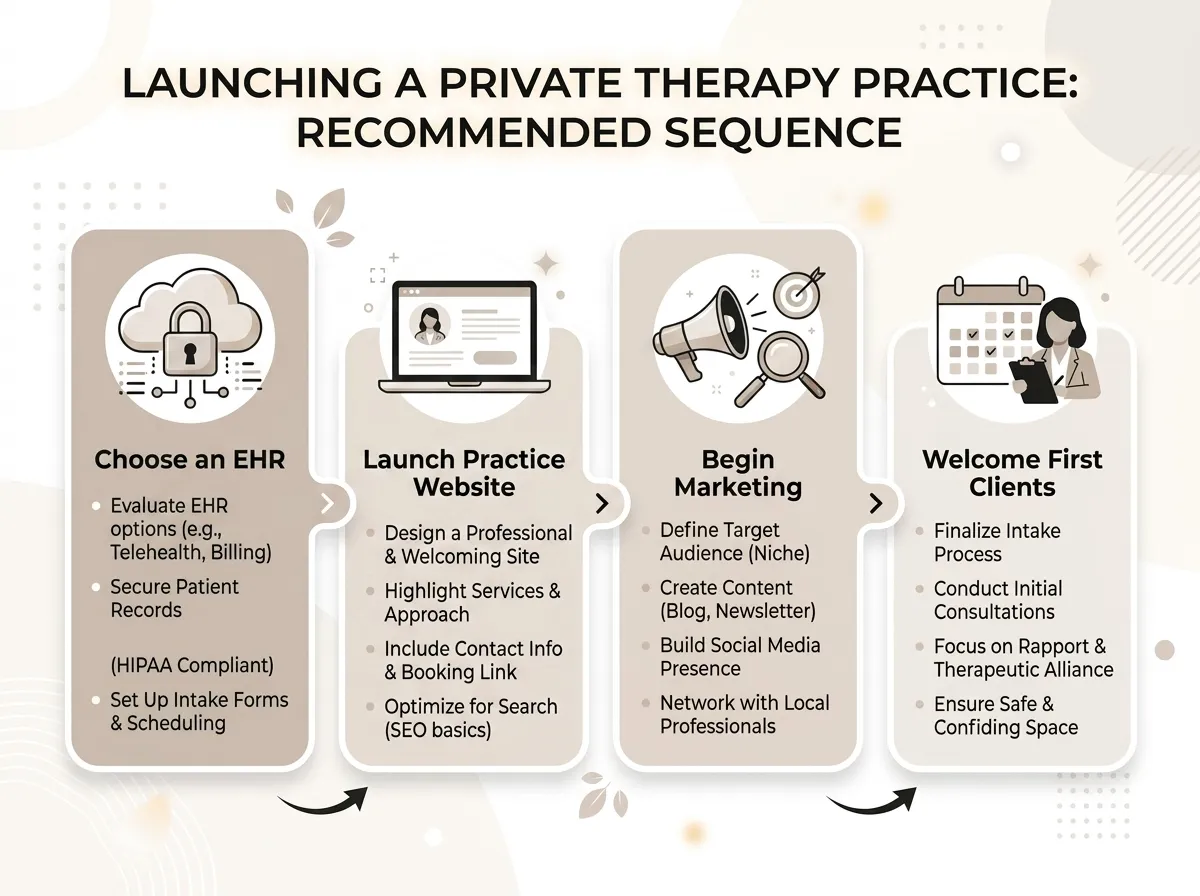
New practice owners ask us this constantly, so here’s the side we take: EHR before your first session, website before your first marketing effort, and in practice both inside your launch month.
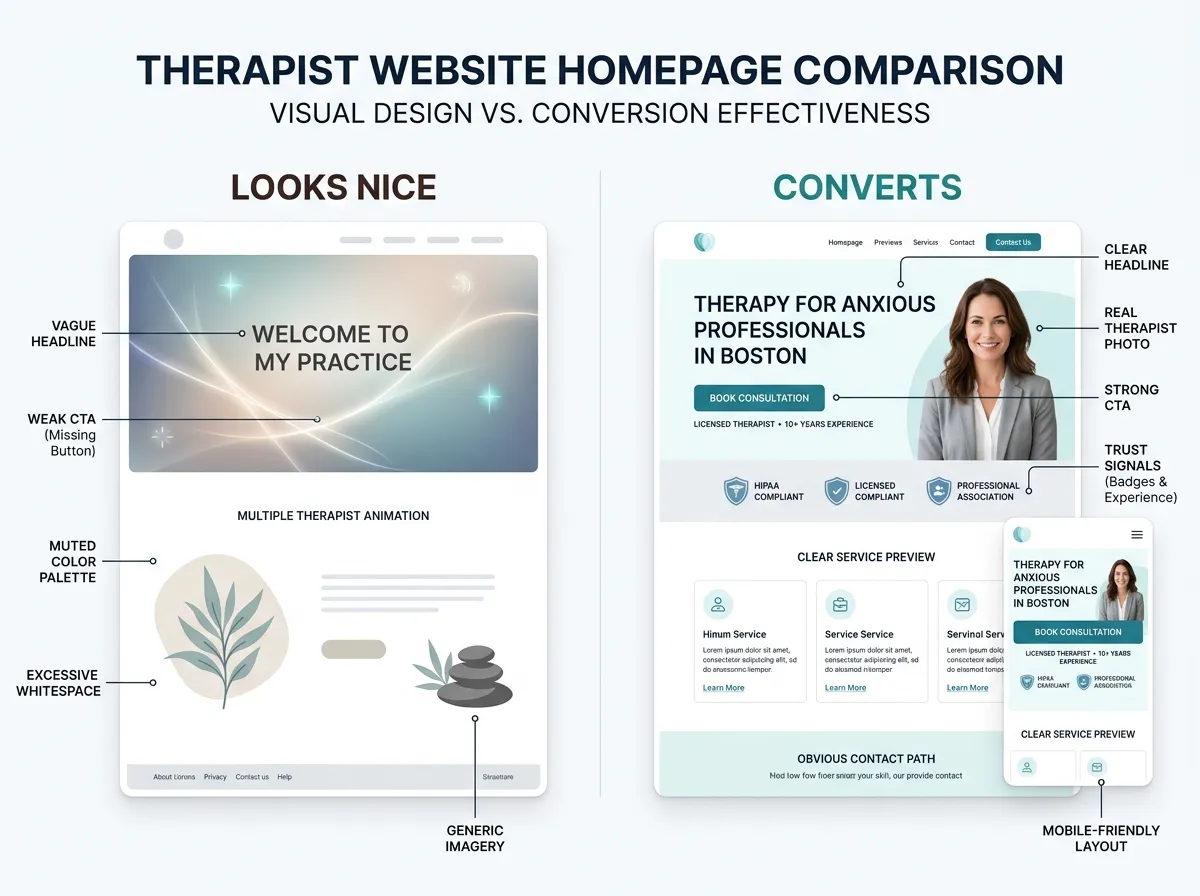
The reasoning is simple. The EHR is your compliance floor; you need somewhere lawful to put records the moment a client exists. The website is your growth engine; it determines whether clients exist at all. Neither replaces the other, and delaying the website “until things settle” is the most common sequencing mistake we see, because a practice with pristine records and an empty calendar is still an empty calendar.
The good news is that the website doesn’t have to be the slow part. Our Website in a Week service takes a therapist site from strategy call to live in seven days, which fits neatly inside the same launch window as your EHR setup. And if you’re still assembling the rest of the launch checklist, our step-by-step practice setup guide puts the EHR and website decisions in order with everything else.
What an EHR won’t do for you
Time for the trade-off, because EHR marketing skips it. An EHR manages demand; it doesn’t create any. The client portal, the reminders, the notes — all of it serves people who already found you. No scheduling feature has ever made a therapist show up on page one of Google.
Also true: paying for software at a caseload of zero stings, and for a few weeks it genuinely is money spent on an empty room. We recommend it anyway, for the same reason you sign an office lease before furnishing it, but pretending there’s no dead-money period would be dishonest.
Where clients actually come from is the part we work on all day: a site that ranks for your specialties, loads fast, and makes booking feel safe. The EHR then catches what the website converts. They’re two halves of one funnel, and most new practices fund the back half first because it’s the half vendors advertise.
How to choose one without losing a month
Don’t demo eight platforms. Shortlist by your three non-negotiables (insurance billing, telehealth, portal quality — whatever yours are), demo two, and pick. Our walkthrough on how to choose a therapy EHR gives you the evaluation checklist, and the full comparison of the best EHR systems for therapy practices covers the current field so you can skip the tab-hoarding phase.
One rule as you compare: verify the vendor signs a BAA before you look at a single feature. No BAA, no shortlist, no exceptions.
FAQ: therapists and EHRs
Is it legal for therapists to keep paper records?
Can I use Google Docs or Sheets for therapy notes?
What does an EHR cost for a solo therapist?
Do private-pay therapists need an EHR?
Where to go from here
Get the EHR set up this week; it’s an afternoon of work that protects every session after it. Then point the same energy at the half of the funnel that actually fills your calendar. If your website isn’t ready to do that job, start a website inquiry and we’ll give you a straight answer on what it needs.