Picture the admissions desk at a mid-size facility on a Friday afternoon. Two hospital discharges pending. A mother on hold about her adult son. A probation officer waiting on paperwork, and a website inquiry from 90 minutes ago that nobody has claimed. None of these people can wait until Monday, and none of them should depend on whose memory holds up. That’s the job a CRM for rehabilitation centers exists to do.
What a CRM for Rehabilitation Centers Handles
A CRM for rehabilitation centers manages everything before intake: inquiry calls and web forms, clinical screening, insurance verification, referral-source tracking, family communication, and follow-up. The admissions team works from one shared record per prospective admission, which becomes a complete file the EHR inherits on admission day. The EHR owns care; the CRM owns the path in.
A solo therapist can run intake from an inbox; we’ve written separately about when solo practices need a CRM, and the answer is usually never. A facility can’t, for reasons that have nothing to do with software preferences. You have multiple admissions coordinators covering phones across shifts. Empty beds carry a real daily cost. Referents expect callbacks. And the person who called this morning ready to enter treatment may feel differently by Thursday, so response speed isn’t one metric among many. It’s the whole game.
Facility admissions is a team sport played against the clock. Teams need a shared board.
The Admissions Pipeline, Stage by Stage
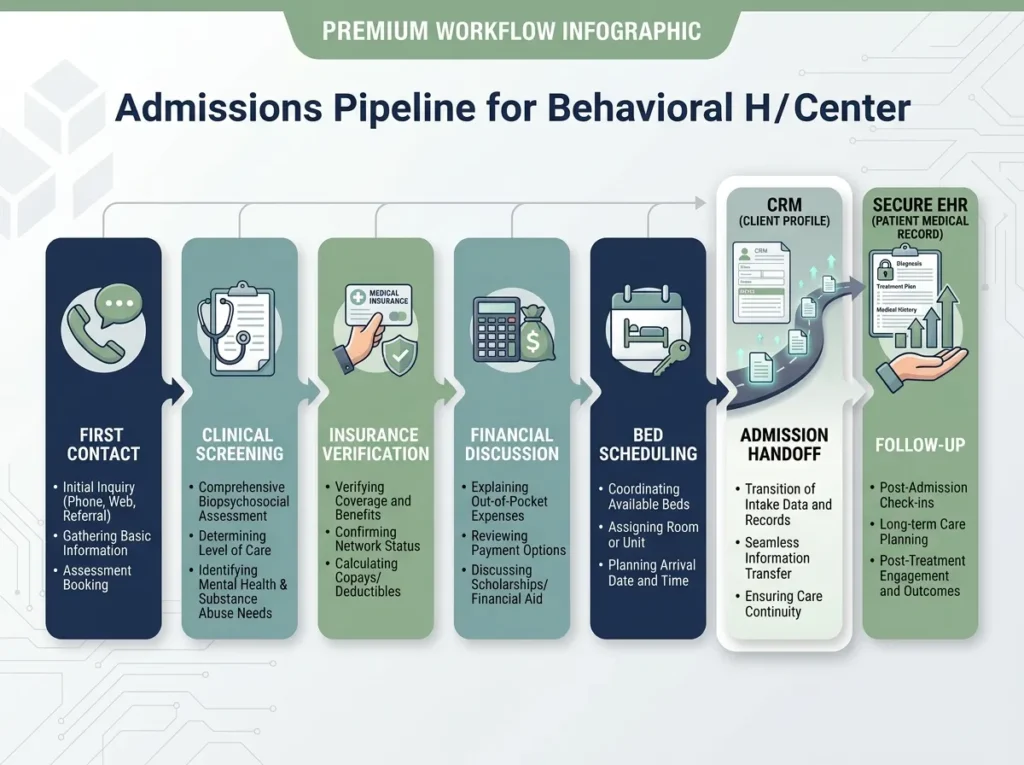
Most facilities run some version of these seven stages, whether or not they’ve written them down:
- First contact: a call, form, or chat. Capture the source and the caller’s relationship to the prospective patient before anything else.
- Clinical screening: presenting needs, level of care, exclusion criteria.
- Verification of benefits (VOB): coverage confirmed and documented, because “we’ll figure out insurance later” sinks admissions.
- Financial conversation: the out-of-pocket picture, stated plainly.
- Bed date and logistics: travel, what to bring, who’s driving.
- Admission handoff: the CRM record becomes a pre-admission chart in the EHR, with nothing re-typed.
- Follow-up: deferrals, no-shows, and waitlist contacts worked on a schedule, not on guilt.
The value isn’t the list. It’s that every open inquiry sits at a named stage with a named owner, so the Monday pipeline review asks “what’s stuck at VOB?” instead of “does anyone remember that call from Thursday?”
Referral-Source Tracking Is Where the Money Is
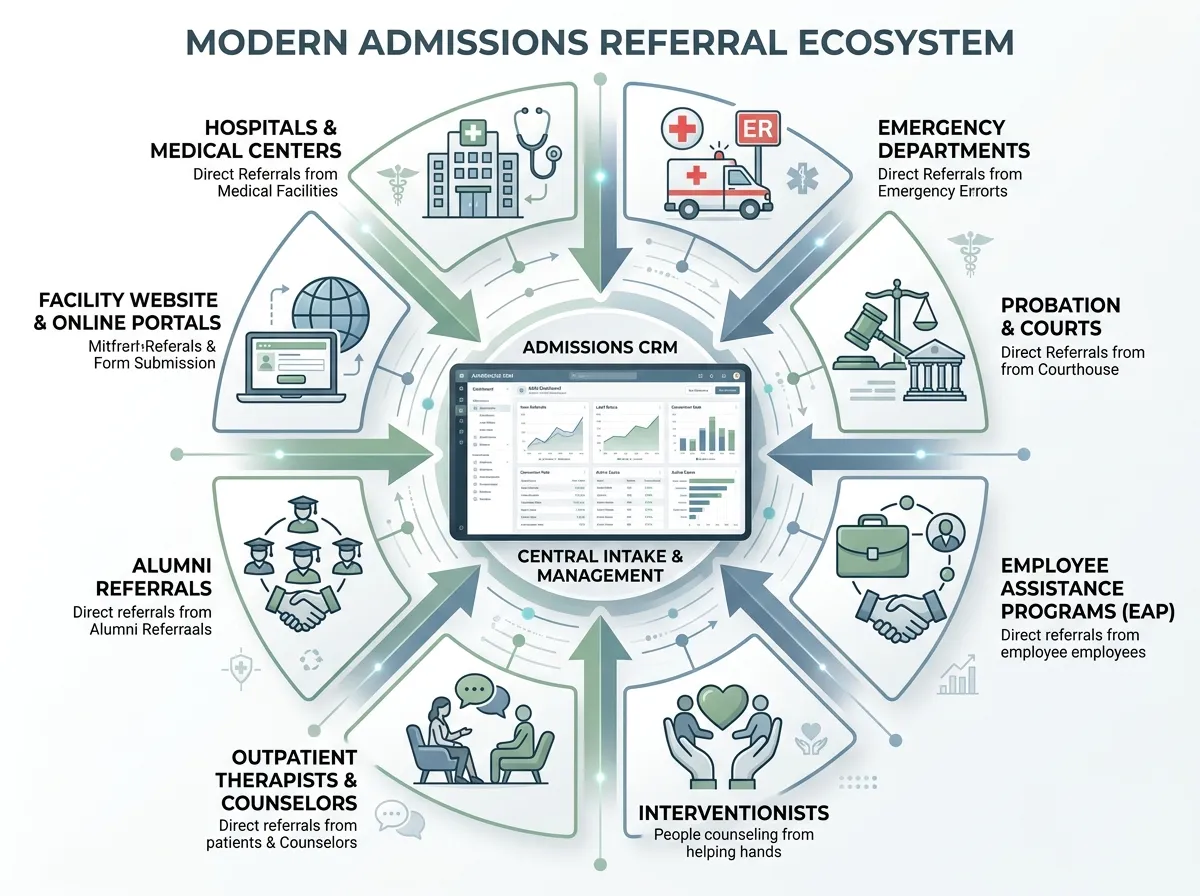
Admissions come from somewhere specific: hospital discharge planners, ER social workers, courts and probation officers, EAPs, interventionists, outpatient therapists, alumni, and your own website. A CRM makes you record which one, every time, at first contact.
Do that for six months and you can answer questions most facilities only guess at. Which hospital sends the most admissions — and which sends inquiries that never convert? Is the EAP relationship worth the quarterly lunch? Our opinion: if you configure only one report in the whole system, make it admissions by referral source. It tells you where the next marketing dollar goes and which referent relationship needs repair before it goes quiet.
Two notes from the field. Closing the loop with referents (a status update within consent limits) is what keeps hospitals referring, and a CRM can put that courtesy on a schedule. And the website is chronically under-credited in these reports: organic-search admissions get logged as “self” or “called in,” which quietly erases the channel’s numbers. Getting that attribution right is half of what our SEO and digital marketing work involves. The honest caveat: a stronger web presence raises inquiry volume, and if the admissions desk is disorganized, more volume makes things worse. CRM discipline first, then turn up the traffic.
Family Contacts Break Normal CRM Logic
In most industries, the lead is the buyer. In behavioral health, the first caller is often a mother, a spouse, or an attorney — not the person who’d be admitted. Generic CRMs handle this badly because their data model assumes one contact per deal.
What you need instead:
- Separate contact records for the family member and the prospective patient, linked to a single admission opportunity
- A consent field that governs who may be told what, visible on every screen
- One named owner per family thread, so the mother who has called three times isn’t retelling her story to a third coordinator
- Scripts for the hardest moments, like a family member calling for a status update the facility isn’t permitted to give
That last point deserves emphasis. Once someone is admitted, what staff can even confirm to a relative is constrained by consent, under HIPAA and more tightly still under Part 2. Which brings us to the part of this decision most vendors underplay.
Part 2 Makes Marketing Automation Riskier Here
Substance-use treatment records sit under 42 CFR Part 2, a federal confidentiality rule stricter than HIPAA’s baseline. It protects any information that would identify someone as having, or having had, a substance use disorder. The 2024 final rule aligned parts of it with HIPAA (a single consent can now cover treatment, payment, and operations), but it also created a patient right to opt out of fundraising contact, and full compliance was required by February 16, 2026.
For an admissions CRM and the marketing stack around it, that means:
- An alumni email list is itself sensitive. Membership on the list discloses treatment history. It can’t sit in a consumer email tool.
- Ad pixels don’t belong on admissions pages. Retargeting scripts can transmit identifying data to platforms that will never sign a BAA.
- Attribution has boundaries. You can count that the website produced twelve admissions; you can’t pipe who they were into an ad platform.
None of this makes behavioral-health marketing impossible. It makes the architecture non-negotiable: the CRM, under a BAA and consent-aware, is the only system that knows who inquired. Marketing tools see aggregate numbers. Facilities that maintain that wall run newsletters, alumni programs, and paid campaigns without ever letting a third party learn who sought treatment. The same wall applies to your website’s forms and analytics; the principles in our breakdown of what the HIPAA rules actually require from a therapy website apply doubly at facility scale.
The Vendors: Purpose-Built vs. Configured
Three realistic routes, based on what’s on the market as of mid-2026:
- Kipu CRM: built for behavioral health. It tracks each opportunity from first contact through admission planning, maintains a referral network with inbound and outbound activity history, and syncs with Kipu’s EMR so admission generates a pre-admission chart instead of a re-typing session.
- Sunwave: merged with Lightning Step in 2025 into a single platform spanning CRM, EMR, and revenue cycle. The pitch is admissions, clinical, and billing under one roof.
- Salesforce, configured: a generalist CRM deployed for behavioral-health admissions with lead routing, VOB tracking, and follow-up automation. Salesforce signs BAAs for covered services (confirm the exact products in scope during procurement), and you should budget for a consultant, because out of the box it knows nothing about beds, referents, or consent.
Our second opinion: for a single facility, the integrated platform usually wins, because the CRM-to-EHR handoff is exactly where data dies and duplicate typing breeds errors. The trade-off is real, though: integration means lock-in. If one module is mediocre, you live with it everywhere, and leaving means migrating admissions, clinical, and billing at once. Multi-site organizations with technical staff sometimes accept Salesforce’s setup cost to keep that flexibility. Whichever route you take, demo against your actual pipeline stages, and re-verify features directly with vendors; this market has consolidated fast.
FAQ: Rehab Admissions and CRMs
What’s the difference between a CRM and an EHR in behavioral health?
Does 42 CFR Part 2 apply to marketing?
Can we use HubSpot or Mailchimp at a treatment center?
Should we fix the CRM or the website first?
Where to Go From Here
A CRM for rehabilitation centers pays off once three things are true: the pipeline stages are named, every inquiry has one owner, and the BAA wall stands between admissions data and marketing tools. Then look at the front door: if the facility’s website is losing inquiries before the CRM ever sees them, start with the Website Inquiry Form and we’ll give you a straight assessment and a custom quote